Chemist warehouse for $281 per vial
1 Like
The Federal Governmnet has extended the shingles catch-up immunisation program for 2 years.
I had no idea that you had to have it in the year of turning 70 (or before)… I had mine at my doc visit last thursday, and he told me about it but he said it was all over after this year. Anyway, I’m done and dusted.
You do not. At least not now.
Zostravax is free for 70-79s. You can get it any time after 50 but you have to pay until 70. You can also get it after 79 if you pay. As I posted, about $180 if you had to pay, current price.
The ‘catch up’ was an initial program introduced to ‘catch’ oldies already over 70 when the Zostravax campaign was rolled out - meant to be temporary. That catch up period has been extended for 2 years to 2023, previously ending this year, so 70-79s can get it free until 2023.
When the campaign ends it is intended everyone get it at 70. That extra 2 years might also be government’s plan to replace Zostravax with Shingrix?
Anyone over 50 can get Shingrix, again as posted, 2 doses at $281 each.
Anyone who has had Zostravax should wait a few years before getting Shingrix if they want Shingrix. A GP will explain it better than an internet forum.
2 Likes
Any ideas why Australian government is persisting with the old Zostavax for shingles when:
- other countries discontinued Zostavax after court case in USA
- Zostavax shown to be less effective in older people (yet Australia still subsidises and recommends it for 70-79 year olds)
2 Likes
Cost is most probable. There is also a somewhat Orwellian handshake that requires the drug manufacturers to apply for PBS and thus being covered further. Sometimes the government in its infinite wisdom taps them on the shoulder to do so, and other times it stands back.
There may also be an impact from the global supply chain still ramping up, and so delaying it on the manufacturer side.
edit: for those interested in the lawsuit, have a read from one of the lawyers and make your own conclusions on merit.
2 Likes
Note Zostravax is manufactured by CSL brand Seqirus.
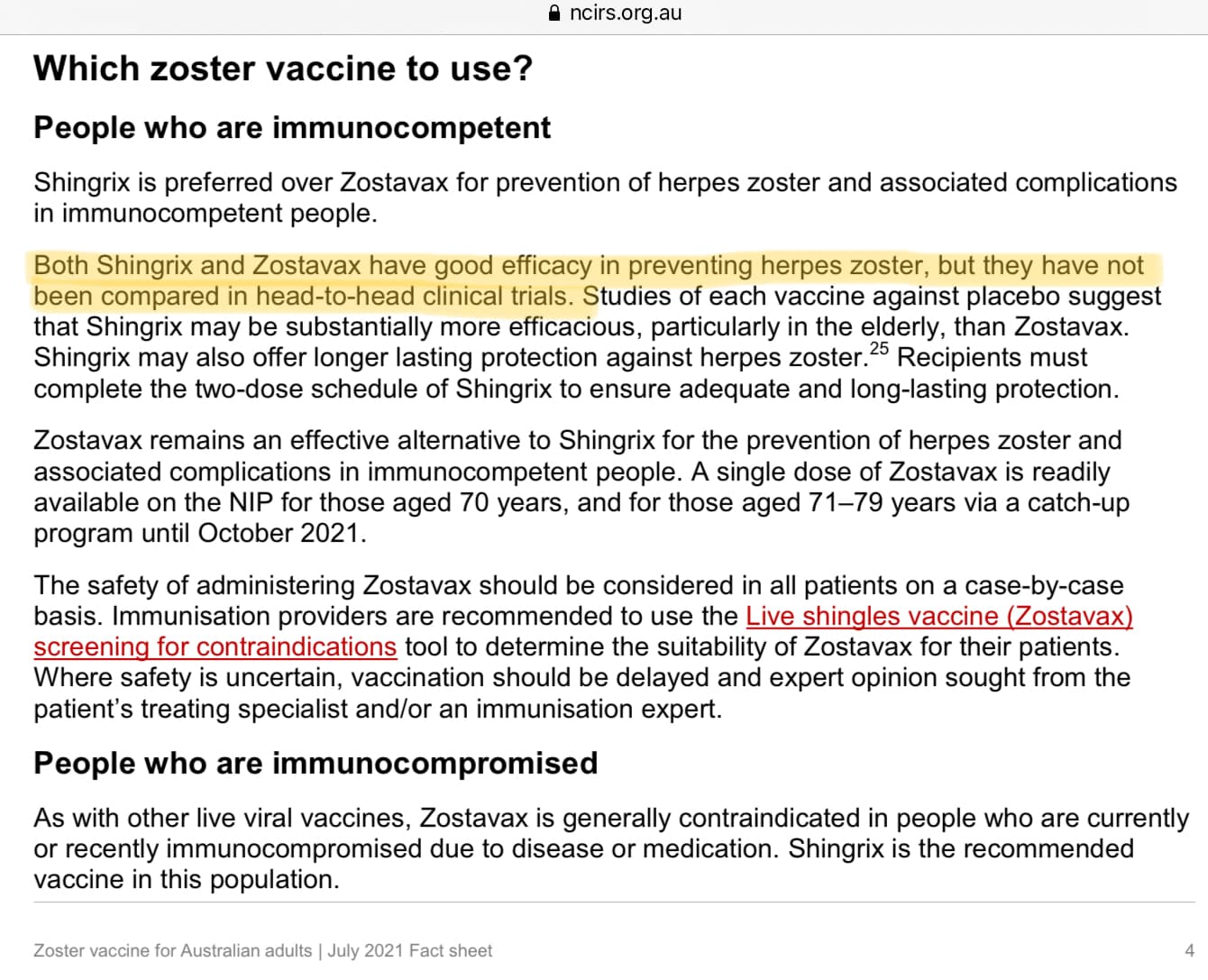
The current medical advice would appear to have avoided making a single recommendation. Both vaccines are considered to have good efficacy.
Note that there has been a recent extension of the end date for the catch up vaccination program.
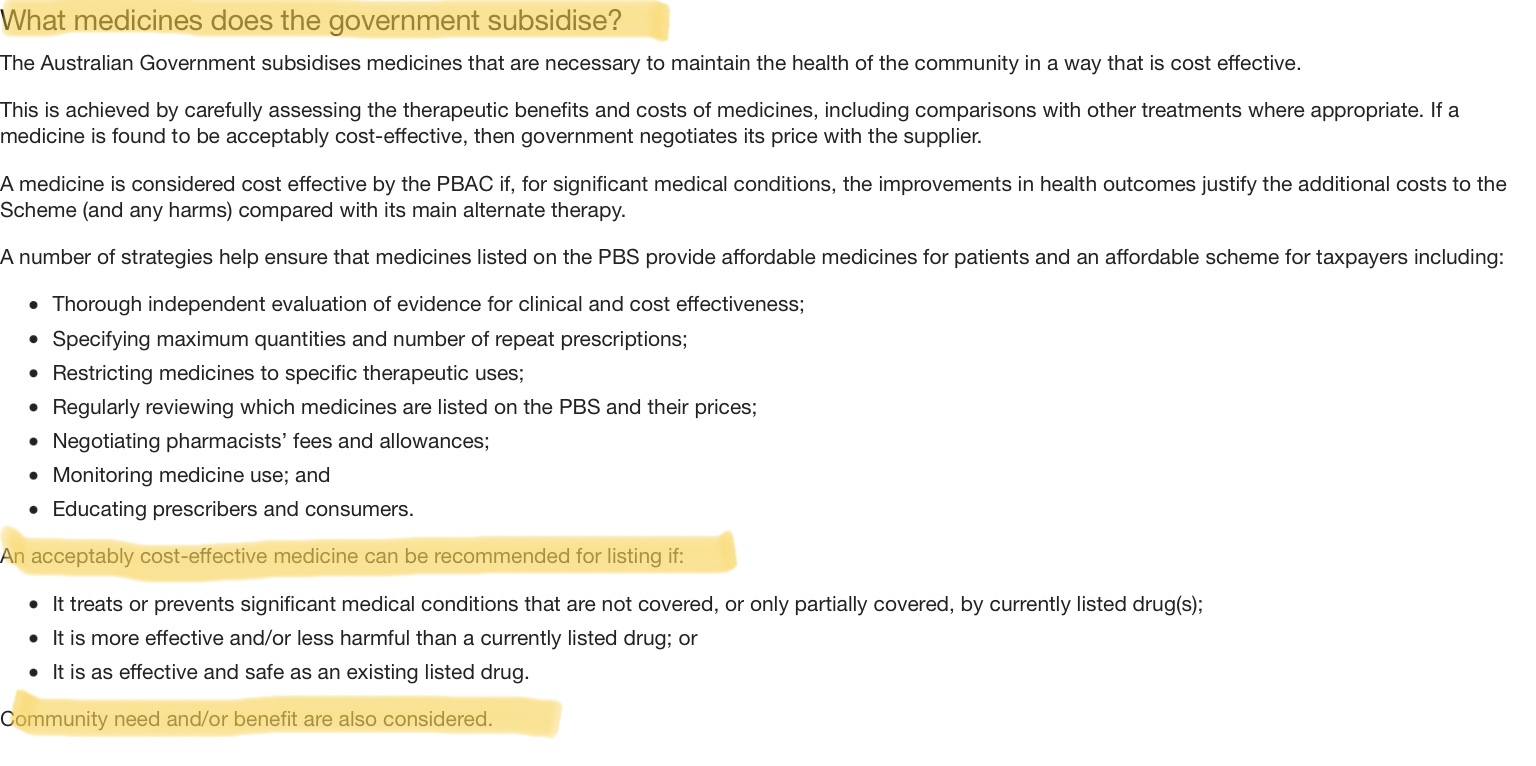
PBS items are subject to a cost benefit test. The Minister for Health has made numerous recent announcements of additional benefits or programs. There is discretion beyond immediate economics.
Apologies if this only explains how the system is supposed to work and not the why. We do have access to vaccines of which one is low cost to the patient.
1 Like
Chuckles. I believe the definition of ‘good efficacy’ for basic WHO approval is 50%. Zostavax is 51% (67% for PHN) and Shingrix >90% according to the US CDC.
In the absence of a head-to-head clinical study I already voted with my pocketbook as noted in prior posts.
2 Likes
It’s been a very enlightening topic.
We will need to do the same, having the benefit of the discussion in the topic for guidance. The chances of a change in Ministerial heart appear slim.
2 Likes
GSK no thanks. I cannot use the PBS shingles vaccine and the one I can is a GSK one with no PBS means close to $600 for the two. Why? I think because GSK forgot to include in their submission the benefits for immuno-suppressed people and indigenous people I think over 51. I told them, did they care? Who knows?
Probably not.
2 Likes
Please note your post has been moved to a topic specifically discussing the GSK vaccine, cost and availability.
Thank you for sharing the observation on the supply of the GSK shingles vaccine. It’s assumed the advice on the suitability of the PBS funded vaccine is from one’s medical specialist. One of the oft quoted complaints concerning the PBS is a lack of transparency of the review and acceptance process.
As to who might be best to look to for the reasons the outcome is not as desired:
- Do we know what GSK included in each of its submissions?
- What did the TGA assess and determine when accepting the product as an approved medication?
- What did ATAGI consider and advise in respect of using the GSK product as part of the national immunisation program?
- What did the PBAC consider and how did it reach its decision to not recommend adding the product to the PBS?
At the end of the process there is a Government rubber stamp, Federal Minister for Health? The responsible minister may have along with the final say some discretion to vary what is recommended. It may prove informative to look back in time to when the GSK vaccine was first approved for use in Australia, or the free immunisation program extended to find which minister.
Background on the approval process and PBS in general.
‘The Pharmaceutical Benefits Scheme: a quick guide – Parliament of Australia
For those interested in Shingrix it is worth reading prior posts. As for the comments on GSK there are two important bits as I see it, the first being ‘how good is Shingrix?’
The second bit is that it is expensive and GSK is pushing it.
A guess is that applying to add it to the PBS and/or NIP* would probably result in having to negotiate their price. Those who can afford it and are aware of it will be happier as well as able to buy a superior vaccine thus supporting GSK profit goals. I could think of little else to back government’s statement that At this stage, the manufacturer has elected not to have Shingrix considered for supply through the NIP.
* NIP → National Immunisation Program
I’m immuno compromised. Ten days ago I was told to visit a tropical diseases specialist who viewed the 25 blood tests and associated test results for which I’d recently provided samples. The specialist wrote a script for a Pneumococcal vaccine. Ok, I need this to move to the next stage of my treatment. There was some surprise when the pharmacist gave me a iv Chicken pox vaccine, which I had as a child and also an iv Shingrix dose. No Pneumococcal vaccine. $60.00 was asked until I showed my pension card which then dropped to $14.00.
I’ve since been back to the Pharmacy and collected a double dose of Stromectol. I guess its the Pneumococcal vaccine, no explanation.
No explantion.
No its for worms, my guess is that is what the tropical diseases specialist identified. Did this doctor offer no explanation of what they were prescribing?
If a pharmacist doesn’t offer you explanations with any new drug, whether prescription or not, you should ask:
- what it is for,
- how to take it,
- what side effects to look out for and
- if it has any interactions with other drugs you are taking.
It is their duty to to give such explanations as part of the service.
2 Likes
Thanks. Yes precisely.
I recall we’d gone beyond the 14 minutes consultation with other business.
Ironically if not so seriously, 36 hours after the vaccs I had emergency surgery after which the surgeons were concerned about a constant mild fever. Pumped me with iv antibiotics for 3 days even after I told them of the double vaccs I’d received.
Apologies, a bit off topic. I do however worry about the level of care in public hospitals.
This seems unusual to me. I have given a few vaccinations in my day but am not an expert. It is possible that the information you have provided is inaccurate. It certainly seems appropriate for the immunocompromised to take the advice of a tropical or infectious diseases specialist regarding immunisations, and if you have been given different immunisations to their advice I would let them know. As far as I am aware, chickenpox vaccine is a live vaccine and is not generally given to people who are immunocompromised because of the risk of complications such as chickenpox. I think that Shingrix is said to be safe in the immunocompromised, but to my knowledge it is still not covered by the Government and would cost a lot more than $60. I also don’t see the logic in having both chicken pox vaccine and Shingrix. I would suggest that, because of your immunocompromised status, you double check with the pharmacy as to what vaccinations you received and contact your specialists or GP this week, especially if you received a live vaccine.
3 Likes
Hi @Sj2, there seems to be confusion over what your medical practitioner may have prescribed in relation to current conditions you have or to protect against future common infections.
The Commonwealth government keeps records of vaccinations administered to Medicare card holders. This information is available through MyGov and should be accessible by your medical practitioner.
As there appears to be confusion over the treatment provided by your medical practitioner, it is suggested that on your next visit you ask what has been prescribed and for what reasons. (e.g treat an existing ailment or for preventative health protection). Hopefully this resolves any confusion or questions you may have.
3 Likes
I am immunocompromised and with the hospitalisation and deaths of Australian immunocompromised patients given Zostavax, I paid the extra for two doses of Shingrix when I was in my early 50s. With this risk in addition to the long-term health consequences of a Shingles infection, it is a travesty that Shingrix is not subsidised on the PBS for all severely immunocompromised patients, irrespective of age.
5 Likes
Here is the last time Shingrix was considered by the PBS.
There is much more to it but essential it isn’t cost effective:
7 PBAC Outcome 7.1 The PBAC did not recommend the listing of the varicella zoster virus vaccine (HZ/su) on the National Immunisation Program (NIP) for the prevention of herpes zoster in adults aged 60 years, with a five-year catch-up program. The PBAC considered that there was some uncertainty in the magnitude of the clinical benefit, that the incremental cost-effectiveness ratios (ICER) were highly uncertain and that the estimated financial impact was high and uncertain. Given the large opportunity cost, the PBAC considered more conservative cost-effectiveness analyses were required.
I am sure we would all like more drugs listed but I think we have to accept that money should be spent in the best way possible.
3 Likes
It seems as much GSK’s profit motive as our government’s will/funding.
From one of my prior posts
Have you scoped the difference between immunisation compared to treatment and how does it compare? Keep in mind 51% versus >90% effective.
3 Likes